
A Multinational Survey Audit by JACIE Quality Managers Committee and GoCART Coalition
Sections:
- Summary
- Methods
- Results (with figures)
- Discussion
- Conclusion
- Recommendations
- Thanks
1. Summary
Hospitals administering CAR-T therapies are increasingly subject to overlapping inspections from manufacturers, accreditation bodies, and national regulators. This “inspection burden” may hinder efficiency despite strong collaboration across stakeholders.
The international survey by the JACIE QM Committee and GoCART coalition of the EBMT, gathered 185 responses from 142 hospitals in 33 countries. The survey evaluated experiences with systems, training, audits, onboarding, and communication along the CAR-T cell process.
The initial data was presented at EBMT 2025 and a Scientific letter published in HemaSphere in October 2025
Operational burden and fragmented implementation in CAR T-cell therapy: Insights from a multinational survey by the GoCART Coalition and the JACIE Quality Managers Committee
https://onlinelibrary.wiley.com/doi/full/10.1002/hem3.70243
The HemaSphere letter covers a technical overview on the issues raised by the survey and considerable background data. It includes an addendum of the hospitals that completed the survey.
This audit report presents direct findings from the survey, organised by topic and supplemented with comments from survey participants. This level of detail could not be included in the HemaSphere letter due to length restrictions. The longer structure allows greater commentary and discussion, giving clarity to statistics provided in the HemaSphere letter.
2. Methods
2.1 Study Design and Objectives
The survey was designed as a descriptive, cross-sectional survey to assess the experiences of hospitals involved in delivering CAR-T cell therapy. The primary objective was to identify bottlenecks and burdens within the hospital processes—particularly those linked to regulatory and manufacturer-driven inspections.
2.2 Survey Distribution and Participants
The survey was distributed in late 2024 and early 2025 to CAR-T program leads, quality managers, data managers, nurses, and coordinators across international centres. A total of 185 responses were received from 142 hospitals in 33 countries, representing approximately 3,400 CAR-T infusions annually. Participating countries included a global mix from mostly Europe, but also North America, Asia, and South America, ensuring broad geographical representation.
2.3 Questionnaire Content
The questionnaire included 25 items covering:
- System usability and communication with manufacturers
- Patient preparation and apheresis
- Courier logistics and documentation
- Data sharing and post-product delivery handling
- Training, onboarding, and annual audits
- JACIE and manufacturer inspection overlap
Most questions used Likert scales for quantitative assessment, while several open-ended prompts allowed for qualitative input.
2.4 Data Analysis
Quantitative data were analysed using descriptive statistics. Responses were grouped by thematic area (e.g., "audits", "training", "communication"), and results were expressed as percentages of positive, neutral, or negative experience. Qualitative responses were analysed thematically, and selected illustrative quotes are presented in the results section.
This report covers all responses received, with no weighting given to responses and there may be more than one response from some organisations if Clinical, Collection, Processing and Quality Management all responded.
The study is based on self-reported survey data and may reflect biases of those more engaged or more burdened by the inspection process. Nonetheless, the large sample size and international scope strengthen the external validity.
Comments are a selection from responders.
2.5 Ethical Considerations
No patient data were collected. Participation was voluntary and there was a choice to be anonymous. The study was exempt from formal ethical review.
This study is based on self-reported survey data and may reflect biases of those more engaged or more burdened by the inspection process. Nonetheless, the large sample size and international scope strengthen the external validity.
3. Results
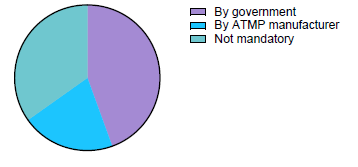
3.1 Hospitals responses whether JACIE is mandatory or not, and if yes, how?
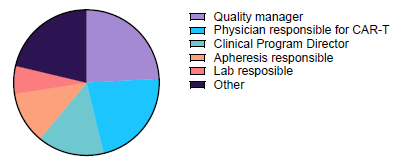
3.2 Respondent Profile
A total of 185 respondents from 142 hospitals in 33 countries completed the survey. The hospitals varied in size and experience, delivering approximately 3,400 CAR-T infusions per year. On average, each hospital worked with three different CAR-T manufacturers, highlighting the need for cross-manufacturer process integration. Respondents included data managers, quality managers, CAR-T coordinators, nurses, and physicians.
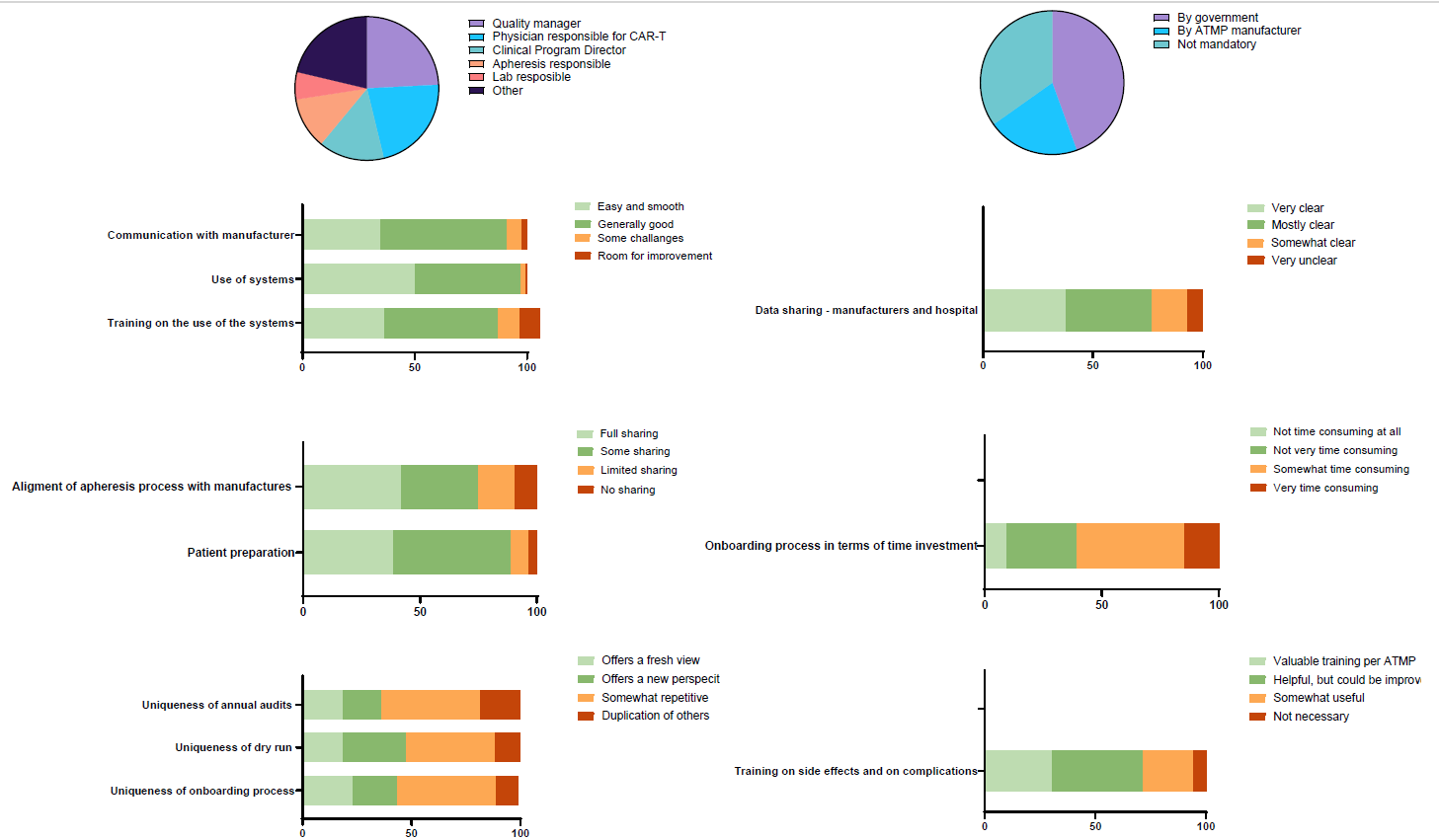
3.3 System Usability and Manufacturer Communication
Hospitals reported high satisfaction with the digital platforms used for booking slots and tracking shipments.
- 93% of respondents rated their experience with systems as positive.
- 92% expressed satisfaction with manufacturer communication throughout the process.
Survey comments on this topic:
“It would be better if the platforms were common.”
“Assigned site managers ensure quick and easy communication.”
3.4 Apheresis and Logistics Variation
Despite general satisfaction, many hospitals cited inconsistency across manufacturers as a barrier to efficiency. Differences in terminology, required documents, and handling protocols were frequently noted.
- 89% rated the apheresis and courier process positively, but qualitative responses indicated growing frustration with redundant steps.
Survey comments on this topic:
“Every process regarding the box is different. For example: digital, paper.”
“Required temperatures differ per manufacturer. It would be great if they could agree on one temperature.”
3.5 Post-Product Arrival and Data Sharing
- 92% rated post-arrival product handling as positive. However, hospitals reported limited data sharing from manufacturers. This lack of transparency was seen as an obstacle to optimizing collection and processing procedures.
Survey comments on this topic:
“Not every company shares the total number of CAR-T cells which makes it difficult to measure the collection efficiency.”
“Very limited information on apheresis material and final product parameters.”
3.6 Training and Onboarding
Respondents reported that while training quality was adequate, onboarding with each new manufacturer was excessively time-consuming:
Survey comments on this topic:
“It would be great, when you're JACIE accredited for CAR-T, that the company reduces the amount of work for the centres.”
“Onboarding should focus more on product-specific aspects, not general training repeated every time.”
Similarly, views on annual audits varied:
- Some manufacturers accepted JACIE accreditation.
- Others repeated full inspections, leading to duplication of effort.
Survey comments on this topic:
“JACIE audit covers the manufacturer, so a manufacturer audit is not beneficial.”
“Some companies… just check JACIE and HTA license. Others re-audit and complete checklists again—it’s frustrating and a waste of time.”
3.7 Harmonization and Recommendations
A strong theme across open-text comments was the need for harmonization:
Survey comments on this topic:
“Eighty percent of the process is the same for different products. Focus should only be on differences.”
“Align procedures of different products to a more unified process. Very time and staff consuming to adjust to each company.”
Respondents advocated for a centralized or standardized approach, with JACIE accreditation acting as a sufficient baseline for process acceptance.
4. Discussion
This multinational survey offers a unique insight into how hospitals across diverse healthcare systems experience the operational burden of CAR-T therapy delivery—particularly with regard to inspections, onboarding, and compliance with differing manufacturer and accreditation requirements.
4.1 A high level of satisfaction, but underlying strain
While overall satisfaction with systems and communication was high (over 90% positive responses), respondents consistently reported fatigue with redundant processes. Variability in documentation, terminology, temperature requirements, and logistics creates friction in daily workflows and undermines efficiency. This suggests that operational excellence in CAR-T delivery is no longer limited by clinical readiness, but by logistical fragmentation.
4.2 The multiple audit problem
A recurring issue was the duplication of audits. Many respondents noted that JACIE accreditation should, in principle, suffice to meet manufacturer and regulator expectations. However, several manufacturers continue to conduct full-scale audits, often requiring time-consuming checklists and revalidation of well-established procedures. While some manufacturers have started to streamline their checks, the inconsistency adds pressure to bedside and support staff.
This aligns with concerns raised by healthcare quality scholars around “inspection fatigue” and the opportunity cost of highly skilled professionals being diverted to non-clinical tasks.
4.3 The case for harmonization
Perhaps the strongest message from the qualitative feedback was the need to standardize what can be standardized. While product-specific nuances are inevitable, 80–90% of procedures (e.g., transport logistics, system usage, courier communication) are similar across manufacturers. JACIE accreditation, is comprehensive and widely trusted, and could serve as a shared baseline to reduce duplication.
This would not only lower the burden on hospitals, but also facilitate better inter-hospital benchmarking, training, and data integration.
5. Conclusion
While 93% of hospitals rated system usability and 92% rated manufacturer communication as positive, open-ended responses highlighted redundancy, lack of harmonization, and inspection fatigue. Respondents supported the idea that JACIE accreditation should suffice for many aspects of quality oversight. Significant variation across manufacturers—particularly in onboarding and auditing practices—was identified as a major barrier.
The growing inspection burden calls for harmonization of processes across manufacturers. Stakeholders should focus audits on product-specific differences, recognize JACIE standards where applicable, and streamline communication and documentation systems. Standardization would reduce staff workload, minimize duplication, and improve efficiency in the CAR-T process.
Hospitals delivering CAR-T therapies face an increasing inspection burden that often includes overlapping audits, repetitive training, and inconsistent requirements from manufacturers. While collaboration with industry remains strong, the lack of harmonization is viewed as a barrier to efficiency and quality improvement.
Our findings suggest that:
- Hospitals overwhelmingly support JACIE as a core accreditation standard.
- Manufacturers should focus audits on product-specific differences only.
- Shared digital platforms and standardized training materials could reduce duplication.
- Data sharing must improve to enable hospitals to optimize apheresis and handling.
- There is a lot of overlap between JACIE and the manufacturers standards
6. Recommendations
For Hospitals:
- Engage proactively with manufacturers during onboarding to clarify existing accreditations.
- Share best practices and standardized workflows with peer institutions.
- Consider forming regional working groups to present unified feedback to industry.
For Manufacturers:
- Align onboarding and audit protocols where JACIE accreditation is present.
- Develop shared logistics templates and documentation formats.
- Invest in universal platforms for ordering, tracking, and communication.
For JACIE and Regulators:
- Promote recognition of JACIE accreditation by industry and national authorities.
- Continue efforts to harmonize CAR-T requirements across the ecosystem.
- Create clear guidance on when additional audits are truly necessary.
7. Thanks
Thanks are to be given to:
- JACIE Quality Management Committee and GoCART Coalition – their support was invaluable.
- Nick van Sinderen, University Medical Centre Cologne Germany, and Julie Dolva, University Hospital Oslo, Norway, for initial development of the survey and first draft data review.
- Caterina Riillo, University Medical Centre Utrecht Netherlands, for detailed data analysis and provision of graphs.
- Jürgen Kuball, University Medical Centre Utrecht Netherlands and GoCART Coalition, for invaluable support throughout the survey process, and negotiating the writing and publishing of the Scientific Letter.
- Christian Chabannon, GoCART Coalition, Tuula Rintala, GoCART Coalition, Christof Scheid, University Medical Centre Cologne Germany, and Suzanne van Dorp, Radboud University Medical Centre Nijmegen Netherlands, for their input and support.