
Title: Between Immunosuppression and Immune Control: Managing Severe GI-GVHD and Intestinal PTLD After Allogeneic Stem Cell Transplant
Submitted by Giulia Losi and Nicola Polverelli
Physicians expert perspective:
Nicola Polverelli, Head of the Unit of Bone Marrow Transplantation and Cell Therapies, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy
Giulia Losi, BMT physician at the Unit of Bone Marrow Transplantation and Cell Therapies, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy
Nurses expert perspective:
Chiara Giacon, Research Nurse at the Unit of Bone Marrow Transplantation and Cell Therapies, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy
A 62-year-old patient with myelodysplastic syndrome with excess blasts according to ICC 2022 (IPSS intermediate-1, IPSS-R intermediate, IPSS-M high) underwent allogeneic stem cell transplantation (allo-HSCT) from an HLA-matched sibling donor after a treosulfan/fludarabine (FT10) reduced-intensity conditioning regimen. Bone marrow–derived HSCs were infused, and GVHD prophylaxis consisted of cyclosporine and methotrexate. Neutrophil and platelet engraftment occurred on days +16 and +22, respectively. From day +28, the patient developed severe acute GVHD with predominant intestinal involvement, classified as overall grade IV according to MAGIC criteria (skin stage 3, upper GI stage 1, lower GI stage 4, liver stage 0). Clinically, he presented with diffuse erythema, high-volume watery diarrhea (up to 5 L/day), electrolyte abnormalities, anorexia, weight loss, and prolonged need for parenteral nutrition. Despite prompt initiation of first-line therapy with methylprednisolone 2 mg/kg/day, GI-aGVHD was steroid-refractory after five days, requiring sequential rescue strategies.
- Which of the following is the current standard second-line therapy for steroid-refractory aGVHD?
A. Vedolizumab
B. Ruxolitinib
C. Mycophenolate mofetil
D. Extracorporeal photopheresis
Second-line treatment with ruxolitinib was started, but dose reductions were required due to progressive thrombocytopenia. After 14 days without adequate clinical improvement, extracorporeal photopheresis (ECP) twice weekly was added. Multiple infections due to multidrug-resistant organisms led to definitive discontinuation of ECP and need for systemic broad-spectrum antibiotics. Only a partial response was achieved. The patient subsequently received three administrations of fecal microbiota transplantation (FMT) with no benefit, followed by four doses of mesenchymal stromal cells (MSC). Compassionate-use vedolizumab was considered but ultimately not pursued for unavailability.
Approximately five months post-transplant (day +163), he developed fever, vomiting, and acute abdominal pain, while still experiencing persistent diarrhea. CT scan documented suspected intestinal ischemia, and exploratory laparoscopy revealed an ulcerated small-bowel segment, which was resected. Histopathology confirmed EBV-positive diffuse large B-cell lymphoma (DLBCL), consistent with monomorphic PTLD, stage IV, with exclusive intestinal involvement and no additional lesions on PET-CT. EBV-DNA remained persistently undetectable.
- After reduction of immunosuppression, which therapy represents the recommended first-line pharmacologic treatment for CD20-positive EBV-driven monomorphic PTLD?
A. R-CHOP chemotherapy
B. Ganciclovir antiviral therapy
C. Rituximab monotherapy
D. Brentuximab vedotin
Given preserved clinical stability, the patient received rituximab 375 mg/m² weekly for four doses, achieving radiologic disease control. However, despite multiple therapeutic lines, the severe GI-aGVHD persisted, with ongoing high-volume diarrhea (2 liters per day) and dependence on intravenous fluid support.
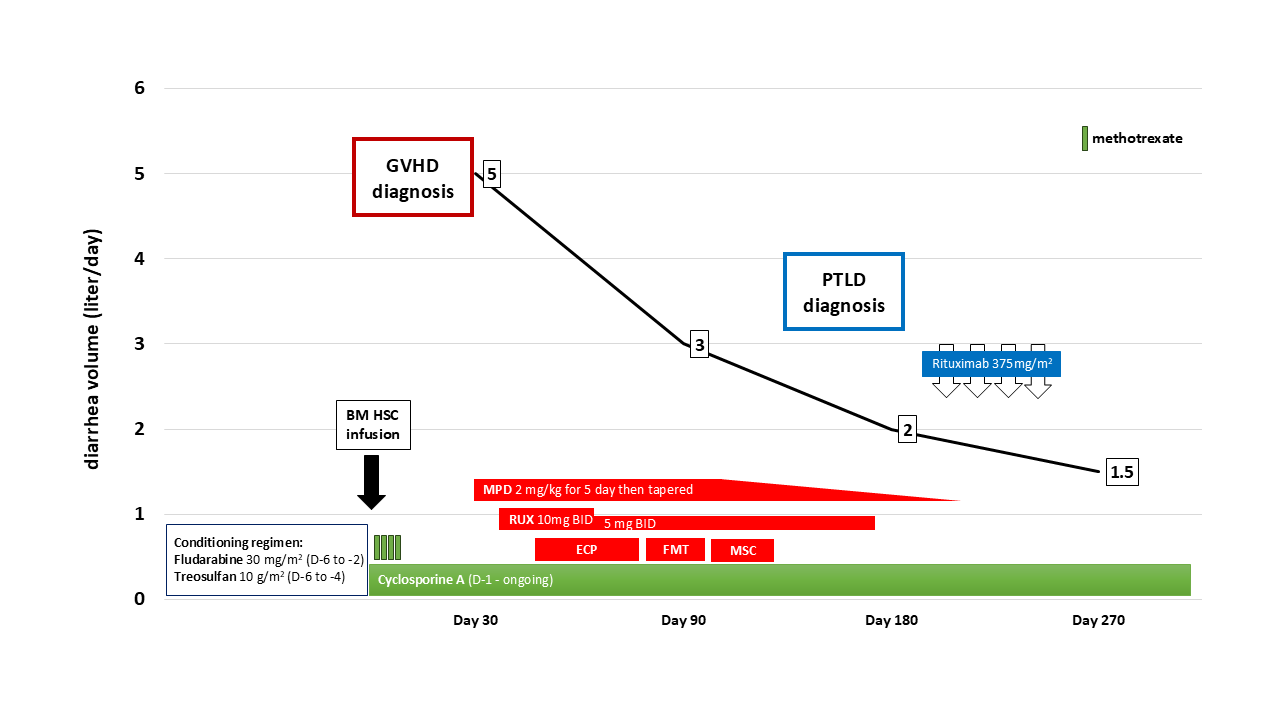
Abbreviations: D: day; BM: bone marrow; HSC: hemopoietic stem cell; GVHD graft-versus-host disease; PTLD: post-transplant lymphoproliferative disorder; MPD: methylprednisolone; RUX: ruxolitinib; BID: twice a day; ECP: extracorporeal photoapheresis; FMT: fecal microbiota transplantation; MSC: mesenchymal stromal cells.
Expert Perspective by Giulia Losi and Nicola Polverelli
This case illustrates the coexistence of two severe post-transplant complications, refractory gastrointestinal acute GVHD and intestinal monomorphic PTLD, both driven by profound immune dysregulation and both associated with high mortality.
Acute GI-GVHD remains among the most challenging complications after allo-HSCT, frequently leading to life-threatening malabsorption, fluid imbalance, and infectious morbidity. Recent Italian data from 2023 transplant activity reported a substantial decline in overall acute GVHD incidence, with only 9% of cases reaching grade III–IV severity, an improvement attributed to advancements in transplant platforms and prophylaxis. Nevertheless, approximately one-quarter of patients still require second-line therapy. Those with severe lower-GI involvement (stage 3–4) represent the subgroup with the poorest prognosis: they are more often steroid-refractory, display profound epithelial damage with barrier disruption, and exhibit high systemic inflammatory signaling.
Ruxolitinib has become the established second-line therapy for steroid-refractory aGVHD, even if ECP as second line may still have a role. Other approaches - such as MSCs, FMT, or vedolizumab - yield variable response rates and lack uniformity in timing, sequencing, and patient selection. Importantly, no treatment beyond steroids and ruxolitinib currently holds EMA approval specifically for this indication. As in this case, patients frequently require prolonged and intensive immunosuppression, placing them at extreme risk for opportunistic and multidrug-resistant infections.
Among infection-related complications, EBV-driven PTLD is particularly concerning. It typically arises in the setting of profound T-cell depletion and is usually associated with rising EBV-DNAemia, although—rarely, as in this case—PTLD may develop with minimal or absent viremia. While lymph nodes are the most frequently involved sites, primary gastrointestinal PTLD is increasingly recognized, often presenting with ulceration, bleeding, perforation, or obstruction. First-line treatment for CD20-positive monomorphic PTLD remains reduction of immunosuppression combined with rituximab monotherapy. EBV-specific allogeneic T lymphocytes is an additional option reserved for rituximab and/or chemo-refractory disease.
One of the greatest challenges in this case was the need to balance two opposing therapeutic imperatives. PTLD management relies on reducing immunosuppression to restore EBV-specific T-cell immunity, while uncontrolled GVHD requires intensification of immunosuppression. Achieving equilibrium is often extremely difficult, and in this scenario, the GVHD ultimately dominated the clinical trajectory.
Despite successful control of PTLD with rituximab and surgical resection, the patient’s prognosis remained determined by persistent severe GI-aGVHD, ongoing cytopenias, fluid and electrolyte instability, and cumulative infectious complications. With no further curative options for refractory lower-GI aGVHD, the clinical team initiated a supportive-oriented care approach, and the patient was discharged.
Beyond the biological complexity, this case underscores the practical and organizational challenges of managing patients with chronic, high-acuity post-transplant complications. Effective care requires a coordinated multidisciplinary team, including hematology, infectious diseases, gastroenterology, clinical nutrition, physiotherapy, and palliative care. Moreover, home-based management remains difficult, as community healthcare systems are often inadequately equipped to sustain the intensity of monitoring and support required, resulting in frequent emergency admissions and fragmented care.
Improving outcomes for patients with refractory GVHD and PTLD will require not only innovative and targeted immunologic therapies but also better integration between transplant centers and community resources. A strengthened continuum of care that effectively bridges hospital-based expertise with home-care capabilities is essential to adequately meet the needs of this highly complex patient population.
Expert Nurses Perspective by Chiara Giacon
The complexity of this case, marked by severe gastrointestinal acute GVHD, multiple lines of immunosuppressive therapy, life-threatening infections, and the emergence of intestinal PTLD, highlights the central and highly specialized role of nursing in the care continuum following allo-HSCT. From early symptom recognition to advanced supportive interventions, transplant nurses act as both clinical sentinels and coordinators of multidisciplinary care, often taking care of patient stability and quality of life.
A key nursing challenge in this scenario is the management of high-volume intestinal losses and associated metabolic derangements. With diarrhea exceeding 5 L/day during peak GI-aGVHD, meticulous monitoring of fluid balance, electrolyte levels, and weight trends becomes essential. Given the risk of rapid fluctuations in potassium, magnesium, and bicarbonate levels, it is essential that nurses ensure the timely administration of prescribed electrolyte replacements and supportive therapies to prevent arrhythmias, neuromuscular complications, and further renal deterioration. Frequent reassessment of mucosal integrity, abdominal signs, and stool characteristics supports both diagnostic refinement and timely escalation of care.
Nutritional vulnerability is another critical domain. As the patient progressed from anorexia to prolonged dependence on parenteral nutrition, nursing responsibilities extended beyond infusion management to prevention of line infections, glycemic control, and daily evaluation of tolerance and metabolic response. The nurse plays a pivotal role in reinforcing safe handling and aseptic technique in both inpatient and outpatient settings, especially when immunosuppression is profound and persistent.
Infection prevention, already central in HSCT care, becomes especially demanding in the setting of multidrug-resistant colonization and prolonged neutropenia or lymphopenia. Strict adherence to isolation protocols, vascular access care, early recognition of sepsis, and antimicrobial stewardship principles are core nursing responsibilities.
The case also illustrates the profound psychological and emotional burden associated with refractory GVHD, in which multiple sequential therapies were undertaken without substantial clinical benefit, generating repeated cycles of hope and disappointment for both the patient and family. Prolonged hospitalization, fatigue, weight loss, and growing dependency further intensified distress, requiring nurses to provide clear, compassionate communication and continuous emotional support as part of holistic care. The subsequent emergence of intestinal PTLD compounded this strain, as the conflicting therapeutic imperatives—escalating immunosuppression for GVHD versus reducing it to control PTLD—created additional uncertainty and fear. Nurses, often serving as the primary interface between the patient and the clinical team, play a crucial role in helping individuals navigate this complex decision-making landscape, addressing concerns, clarifying evolving treatment goals, and advocating for symptom relief and comfort in a context marked by chronic stress and vulnerability.
As the disease course evolved toward supportive-oriented care, the nursing role shifted again to ensuring comfort, aligning clinical goals with patient wishes, and facilitating a safe discharge. Transition to home care is often challenging due to limited community resources equipped to manage complex transplant patients. Nurses act as advocates for continuity, helping arrange hydration plans, wound care, nutritional support, and emergency pathways to avoid unnecessary crises.
Ultimately, this case demonstrates that expert nursing in allo-HSCT is not limited to executing medical plans; it encompasses clinical vigilance, patient education, emotional support, ethical dialogue, and coordination across systems of care. The nurse’s presence—consistent, skilled, and adaptive—remains fundamental in navigating the uncertainties of severe post-transplant complications.
Correct Answers: question 1 – B; question 2 – C.
References:
- Zeiser R et al. Mechanisms and management of acute graft-versus-host disease. Nat Rev Clin Oncol (2021).
- Polverelli N et al. Trends in GVHD Epidemiology, Prophylaxis and Management: The Gruppo Italiano per il Trapianto di Midollo Osseo, Cellule Staminali Emopoietiche e Terapia Cellulare (GITMO) GVHD24 Study. American Journal of Hematology (2025).
- Smallbone P et al. Steroid Refractory Acute GVHD: The Hope for a Better Tomorrow. American Journal of Hematology (2025).
- Shaikh H et al. Outcomes and Prognostic Assessment of Post-Transplant Lymphoproliferative Disorder: 20-Year Experience. Lymphatics (2025).
- Nader Kim El-Mallawany, Rayne H. Rouce; EBV and post-transplant lymphoproliferative disorder: a complex relationship. Hematology Am Soc Hematol Educ Program (2024).
- Mahadeo KM et al. Tabelecleucel for allogeneic haematopoietic stem-cell or solid organ transplant recipients with Epstein-Barr virus-positive post-transplant lymphoproliferative disease after failure of rituximab or rituximab and chemotherapy (ALLELE): a phase 3, multicentre, open-label trial. Lancet Oncol (2024).
- Reiche W et al. Gastrointestinal manifestations, risk factors, and management in patients with post-transplant lymphoproliferative disorder: A systematic review. World J Transplant (2022).
- Shah R et al. Multidisciplinary Management of Morbidities Associated with GVHD. Multidisciplinary Management of Morbidities Associated with Chronic Graft-Versus-Host Disease. Clinical hematology international (2024).
- Proença SF et al. Quality of life of patients with graft-versus-host disease (GvHD) post-hematopoietic stem cell transplantation. Rev Esc Enferm USP (2016).
Future Clinical Case of the Month
If you have a suggestion for future clinical case to feature, please contact Anna Sureda.